Giving birth to your baby may be the most beautiful and unforgettable experience in your life, especially if you prepare for it before your term.
I was preparing myself for the natural vaginal birth with my baby, however I had to do the c-section due to certain conditions. I was traumatized at the thought of not being able to give birth naturally and thought of how much easier it would be if I knew how c-section worked and what the real risks were.
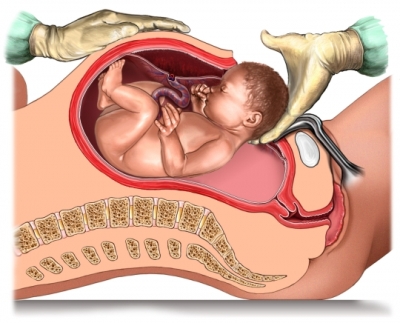
The Surgery:
There are multiple layers that your surgeon must go through before reaching the baby. All in all from the start of surgery, until the birth of your baby is about 5-10 minutes. The doctor will use a combination of sharp instruments and blunt dissection as s/he goes through each layer. You may also hear whirring noises as a machine is used to caterize or burn small blood vessels to prevent bleeding. When the doctor reaches the uterus, you will also hear suctioning. After cutting through the uterus, the amniotic fluid will be suctioned away to make a bit more room in the uterus for the doctor's hands or instruments such as forceps or a vacuum extractor. Your baby is usually engaged in the pelvis, usually head down, but perhaps rear first or breech. Whatever part has entered the pelvis will be lifted out by the doctors. You may feel pressure at this point and some women report feeling nauseated during this intense, but brief moment. Once the head is out, your doctor will suction the baby's nose and mouth for fluids. In a vaginal birth these are normally squeezed out by labor and birth. In a cesarean birth, the baby needs some extra help getting rid of these fluids. If meconium is present there may be extra suctioning required.
However, before you consider the C-section for your baby's birth, you should also weigh the risks. Cesarean birth is major surgery, and, as with other surgical procedures, risks are involved. The estimated risk of a woman dying after a cesarean birth is less than one in 2,500 (the risk of death after a vaginal birth is less than one in 10,000). There are normally serious
medical indications leading you to c-section:
- prolonged labour
- fetal distress
- uterine rupture
- hypertension
- tachycardia
- placental problems
- failed labour induction
- overly large baby
- umbilical cord abnormalitie, etc.
Risks for mother include:
- Infection. The uterus or nearby pelvic organs such as the bladder or kidneys can become infected.
- Increased blood loss. Blood loss on the average is about twice as much with cesarean birth as with vaginal birth. However, blood transfusions are rarely needed during a cesarean.
- Decreased bowel function. The bowel sometimes slows down for several days after surgery, resulting in distention, bloating and discomfort.
- Respiratory complications. General anesthesia can sometimes lead to pneumonia.
- Longer hospital stay and recovery time. Three to five days in the hospital is the common length of stay, whereas it is less than one to three days for a vaginal birth.
- Reactions to anesthesia. The mother's health could be endangered by unexpected responses (such as blood pressure that drops quickly) to anesthesia or other medications during the surgery.
- Risk of additional surgeries. For example, hysterectomy, bladder repair, etc.
- Risk of adhesions.
- Risk to future fertility and babies.
- Risk that future births will have to be surgical
- Maternal death (very rare)
Risks for the baby:
- Higher infant mortality risk: in c-sections which are performed with no indicated risk (singleton at full term in a head-down position), the risk of death in the first 28 days of life has been cited as 1.77 per 1,000 live births among women who had c-sections, compared to 0.62 per 1,000 for women who delivered vaginally
- Wet lung: retention of fluid in the lungs can occur if not expelled by the pressure of contractions during labor
- Potential for early delivery and complications: Pre-term delivery is possible if due date calculation is inaccurate. One study found an increased risk of complications if a repeat elective Caesarean section is performed even a few days before the recommended 39 weeks
As for the
anaesthesia, it is common to use the epidural or spinal anaesthesia during the c-section. Advantages of regional anesthesia include the absence of typical risks of general anesthesia: pulmonary aspiration of gastric contents and oesophageal intubation. Regional anaesthesia is used in 95% of deliveries, with spinal and combined spinal and epidural anaesthesia being the most commonly used regional techniques in scheduled Caesarean section.



 Modesty, and in the Veiled Christ, the original stylistic message is in the veil, but Sanmartino’s late baroque feeling and sentiment permeate the shroud with a movement and a meaning far removed from Corradini’s rules. The modern sensitivity of the artist sculpts and divests the lifeless body of its flesh, which the soft shroud mercifully covers, on which the tormented, writhing rhythms of the folds of the veil engrave deep suffering, almost as if the compassionate covering made the poor limbs still more naked and exposed, and the lines of the tortured body even more inexorable and precise.
Modesty, and in the Veiled Christ, the original stylistic message is in the veil, but Sanmartino’s late baroque feeling and sentiment permeate the shroud with a movement and a meaning far removed from Corradini’s rules. The modern sensitivity of the artist sculpts and divests the lifeless body of its flesh, which the soft shroud mercifully covers, on which the tormented, writhing rhythms of the folds of the veil engrave deep suffering, almost as if the compassionate covering made the poor limbs still more naked and exposed, and the lines of the tortured body even more inexorable and precise.